Reviewing PD Management in Elderly Surgical Patients
With our ageing population and the elderly being in better health in even extreme old age there are greater numbers of acute admissions fit for invasive surgical intervention. Even the healthy aged may have a multitude of medical issues picked up throughout their lives and acute illness can disrupt a fine balance that has been established allowing them to function well outside of hospital.
Given the growing body of evidence that our surgical colleagues do not feel adequately trained to manage the complex elderly, many hospitals now have input from elderly care physicians in surgical patients in some form. At Medway Maritime Hospital we have, since early this year, had a Medical Acute Frailty Service where all admissions through the medical take who are aged over 80 or meet certain other frailty criteria are seen by the team.
We would perform a CGA-based review and make a plan for their immediate management with a longer-term plan through to discharge. I am currently working on a model to establish an Acute Surgical Frailty service so when I had to think of a project for the PD masterclass it seemed logical to use the opportunity to examine management of patients with PD who are admitted under the surgical specialities
I contacted health informatics to get the names of all patients admitted in the preceding year. These included anybody over the age of 80 admitted acutely under orthopaedics, vascular surgery, urology, ENT and general surgery and had a coding diagnosis of PD. This gave me a total of 53 admission episodes to review. Unfortunately getting the notes has been an issue and so the review is ongoing but 25 sets of notes have so far been assessed.
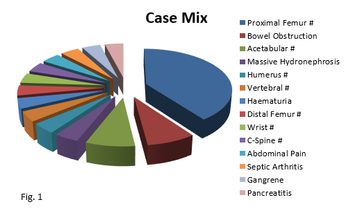
When reviewing the notes I looked for issues with drugs such as incorrect prescribing and missed doses, use of our excellent PD nurses, use of bridging therapy in patients who were made NBM and any other instances of good or poor practice. We had a group of nine males and 16 females with an average age of 85 years. The patients were predominantly orthopaedic, which is understandable given the increased fall to fracture risk in this group, but there was a wide variety of other presentations (see fig.1). The average length of stay was 17.4 days.
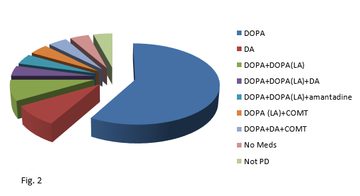
The patients were also on a wide variety of medication regimens although the majority were on single agent sinemet or madopar. One case was on no medications as they had all been recently stopped by their GP with no reason given and another was an incorrectly coded patient with benign essential tremor.
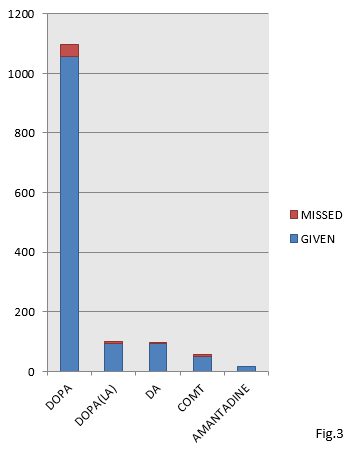
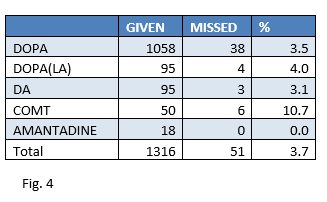
I reviewed all the drug charts to see if drugs had been properly prescribed on admission and to see if any doses had been omitted. All the drug charts reviewed had “Give On Time” stickers on the front and in general adherence to regimens was good. Out of a total of 1,316 doses to be given only 51 were missed. The majority of missed doses were of sinemet/madopar (fig. 3 and fig. 4).
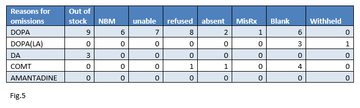
The reasons for missed doses were unfortunately a little disappointing (fig.5). The largest group of missed doses were unexplainable as the box on the drug chart was left blank. This may mean the drug was given and not signed or it may have been missed completely. The next largest group was “out of stock” which is again disappointing as all the drugs required by this cohort of patients are available at all times within the hospital either through the emergency drug cupboard or the supply kept on one of our elderly care wards. All cases where the patient refused or was unable were in cases of acute delirium. This was not documented by the surgical team in most cases but interpreted from comments in the notes such as “acutely confused”. All the missed doses due to NBM were in a single case of bowel obstruction who was receiving palliative care. “Absent” codes were due to patients being in theatre or off the ward for investigations. There was a single omission due to a prescription being incomplete.
Next I looked at the surgical team’s use of our PD nurses. Only just under half the patients (48%) were referred and all the referrals were seen within one working day. On average patients were seen on day five of their admission and had two visits in total (highest was four visits). All the plans were carried out by the team and they were mostly reinforcing of the need for medications to be given, delirium avoidance such as treating constipation etc. and avoidance of dopamine antagonists such as metoclopramide and prochlorperazine. It can be quite difficult to work out from the notes who initiated the referrals but after discussion with our PD nurses it appears the majority come from SaLT (speech and language therapy) and physiotherapy. They also commented that they feel their service is under-utilised in surgical patients and they have the capacity to do more.
I looked at discharge destination for this group and found most patients (13 of 25) were discharged back to their previous residence with no decline in function. Two patients went to rehab with a plan to return to their previous residence, one was repatriated to their local hospital, one was transferred to a tertiary centre for treatment. four patients needed step up in care such as moving in to a residential home or from a residential home to a nursing home and four patients died during the admission.
Finally I looked at examples of good and bad practice. Generally I found that there was good awareness that drugs needed to be given correctly and effort was made to ensure regimens used at home were kept up in hospital. Orthopaedics made the best use of the PD nurses but the service is still underused. It was pleasing to see very few missed doses due to NBM. There was a single case where a patient had severe hypoactive delirium and was unable to take her medications. She was commenced on a rotigotine patch which resolved her delirium within 24 hours. It was just unfortunate that this measure was only used after 72 hours of her not being able to take her tablets. There were two cases of poor practice, both around end-of-life care. Both patients were described as being too unwell to take medications and were left untreated for their final days. Without seeing the patients at the time it is difficult to comment whether or not a parentral treatment such as a rotigotine patch might have given them a better quality of life in their final days but my personal feeling is that it would.
Discussion
I feel that this project has shown, in general, good practice in managing our population of PD patients who need surgical care. Despite this I feel there are some issues that need to be addressed. Firstly I feel a better understanding of delirium is needed. Given how common it is in surgical patients, especially in proximal femur fractures, better teaching for surgical trainees or support from geriatricians is vital. I have found it very difficult to accurately assess the true levels of delirium in this group of patients due to lack of documentation. If surgical teams are not assessing patients routinely for delirium it is unlikely that it is being effectively managed. Missing medications due to delirium leads to loss of function, increases the risk of adverse events such as hospital acquired pneumonia and may prolong the duration of the episode. Given the availability of parentral treatments such as patches there is no excuse for patients being left untreated. The drug omissions section shows that we need to educate staff about facilities in the hospital to obtain the necessary drugs which exist 24/7 and not take the sometimes easier option of just missing the dose and waiting for the pharmacy staff to supply the drug. Finally I would say that all of the above issues could be solved by more input from geriatricians and better use of the PD nurses as we can give advice on drugs, recognising and managing delirium, palliative care in PD and how to make sure drugs are available on the ward and are correctly prescribed.
More Parkinson's Academy Elderly care Projects

'The things you can't get from the books'
Parkinson's Academy, our original and longest running Academy, houses 23 years of inspirational projects, resources, and evidence for improving outcomes for people with Parkinson's. The Academy has a truly collegiate feel and prides itself on delivering 'the things you can't get from books' - a practical learning model which inspires all Neurology Academy courses.